Immediate Risks
Physical
- Perforation of the Uterus and Cervical Lacerations are two of the most common complications of abortion. This is due to the fact that most abortions are by suction aspiration, a procedure where the doctor essentially goes in blind. In future pregnancies these injuries can result in premature births and labour complications.
- Although less common, serious injuries have also resulted from the perforation of the intestine or other organs by an instrument used in abortions. (See Case Study)
Emedicine.com lists the following immediate complications for abortions:
- Pain and/or bleeding
- Infection and low-grade fever
- Hematrometra (a collection or retention of blood in the uterine cavity); uterine perforation; bowel and bladder injury
- Retained products of conception
- Failed abortion
- Cervical shock
SEXUAL DYSFUNCTION: According to research by the Elliot Institute, 30% to 50% of women report experiencing sexual dysfunctions, of both short and long duration, beginning immediately after their abortions. These problems may include one or more of the following:
- Loss of pleasure from intercourse
- Increased pain
- An aversion to sex
- Development of a promiscuous life-style
Psychological
A 1997 Government study in Finland showed that women who have had abortions are four times more likely to die in the next year than those who complete their pregnancies. This is a result of both psychological effects, which result in an increase of suicides and risk-taking behaviour, and an increase in deaths from other medical causes.
In a study of post-abortion patients only 8 weeks after their abortion, researchers found that 44% complained of nervous disorders, 36% had experienced sleep disturbances, 31% had regrets about their decision, and 11% had been prescribed psychotropic medicine by their family doctor. Elliot Institute, PO Box 7348, Springfield, IL 62791-7348. Additional material is posted at www.afterabortion.org.
Long Term Risks
Physical
- Due to the damage resulting from cervical lacerations, women who receive abortions often have difficulty conceiving or carrying future children to term.
- Some abortions cause perforation of the uterus, which usually goes undiagnosed and can result in pregnancy complications and eventually damage to the uterus requiring a hysterectomy.
- Placenta previa in subsequent pregnancies is much more common in women who have had abortions. This can seriously endanger unborn children, leading to malformation and sometimes death.
- Abortion and Cancer: Data indicates that the rates of cervical, ovarian, breast and liver cancer are greatly increased by abortion. Some studies suggest that one abortion increases the chances of cervical cancer by 130 percent, while two increase the chances by 392 percent. The increase in cancer risks for women are due to the violent disturbance of the normal hormonal balances of pregnancy, as well as frequent cervical damage.
Psychological
- (2) A 5 year retrospective study in two Canadian provinces found significantly greater use of medical and psychiatric services among aborted women. Most significant was the finding that 25% of aborted women made visits to psychiatrists as compared to 3% of the control group. (3) Women who have had abortions are significantly more likely than others to subsequently require admission to a psychiatric hospital. At especially high risk are teenagers, separated or divorced women, and women with a history of more than one abortion. Elliot Institute, PO Box 7348, Springfield, IL 62791-7348. Additional material is posted at www.afterabortion.org (4)
- Abortion is significantly linked with a two fold increased risk of alcohol abuse among women. (16) Abortion followed by alcohol abuse is linked to violent behavior, divorce or separation, auto accidents, and job loss… similarly abortion has been linked to higher dug abuse. (Elliot Institute)
“Abortion is Four Times Deadlier than Childbirth.” Elliot Institute, PO Box 7348, Springfield, IL 62791-7348. Additional material is posted at www.afterabortion.org
Links to Further Information on Abortion Consequences:
http://www.youtube.com/watch?v=iH6zN4pMrhw
http://www.lifeadvocate.org/7_97/nation2.htm
Case Report
A 34 year old Indian lady, gravida 6, para 5 with 12 weeks gestation, presented with loops of bowel hanging at the introitus following dilatation and curettage by an unqualified physician. She attended the accident and emergency department of a tertiary referral hospital an hour and a half after the procedure. There was no previous history of abortion or caesarian section. She was not on any contraception. On examination, the patient was very anxious, hypotensive with pulse rate of 120 beats per minute. About four meters of small bowel loops were seen protruding out at vaginal introitus. Full length of bowel loops were bare tubes without any mesentery. Per vaginal examination revealed loops coming through the cervical canal. Palpation of abdomen revealed signs of peritonitis. Given the clinical findings, no imaging or sonogram could be done before the surgical procedure.
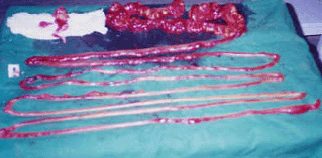
Photograph showing resected coils of intestine
Patient was resuscitated with crystalloids. She had an emergency laparotomy. Perforation was noted at the fundus with loops of jejunum and ileum entering into the uterus. Mesentery was stripped off from the bowel loops at mesenteric border without serious vascular disruption. There was about 500 ml of blood in the pelvis. Large bowel was intact. Remnants of the small bowel loops were clamped and four meters of bowel was resected. End-to-end anastomosis was done with remaining three feet of jejunum and two feet of ileum. Uterine perforation was sutured. Mutilated fetus that migrated during curettage was found at right paracolic gutter. Tubectomy was not done as the patient refused to give consent pre-operatively for permanent sterilization. She recovered well following surgery. On follow-up ultrasonogram, uterus showed no product of conception. Patient was discharged after a week with advice on diet and family planning.
“Uterine Perforation With Subtotal Small Bowel Prolapse – A Rare Complication of Dilatation and Curettage.” JHAS Jan-Mar 2005 http://cogprints.org/4476/1/2005-1-6.pdf
Case Study 2
Case: An 18-year-old gravida I para 0 female presented from an outlying facility I week after elective termination at 18 weeks of gestation with complaints of severe abdominal pain, nausea, and vomiting. Exploratory laparotomy for presumed bowel obstruction revealed uterine perforation and bowel devitalization and necrosis, which required small bowel resection. Fetal bones were discovered within the surgical specimen.
Conclusion: Morbid, even potentially fatal, complications can occur as a result of pregnancy termination. With second-trimester procedures, perforation can result in injury to abdominal viscera from the perforating instruments or even from sharp fetal bony structures.
“Uterine perforation resulting in bowel infarction: Sharp traumatic bowel and mesenteric injury at the time of pregnancy termination.” BNET Research Center Jan 2000
Suicide Rate By Month